
(Note – this is a copy of a post I stuck on my shiny newish blog which, so far, consists solely of gibberings about Covid and vaccines! I need to expand my focus… Posting this here as it has an evolutionary flavour. Looking forward to arguing about Natural Selection for the tenth time!).
I have discussed Geert vanden Bossche’s debatable theories before. Briefly, he argues that mass vaccination in a pandemic ‘selects’ for mutants that escape the immunity conferred by the vaccine, and this threat is reason enough to just stop. He ignores selection for escape of what is loosely, but erroneously, termed ‘natural immunity’, and the enormous health and social costs attaching to the sledgehammering of this nut. Unfortunately for his theories, all variants so far have arisen in poorly vaccinated settings.
Now, Bret Weinstein – who claims to be an evolutionary biologist, yet – attempts, in his podcast and substack, ‘On Driving SARS-CoV-2 Extinct’, to rescue vanden Bossche from the dumpster and brush the banana skins from his shoulders.
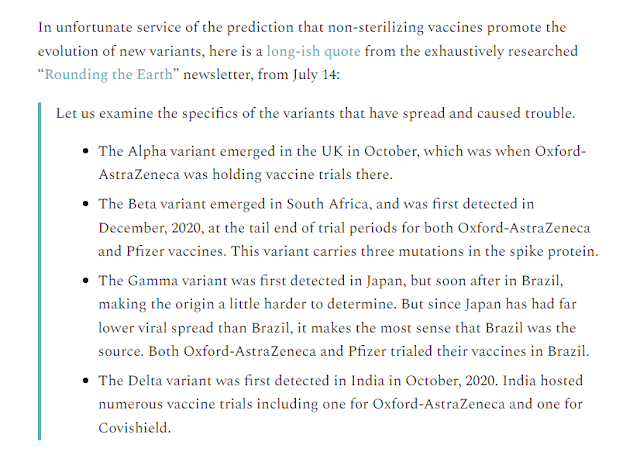
Here’s an excerpt – ‘Rounding the earth’ is the work of one Mathew Crawford:
(I am aware that a properly-conducted review would include links to sources. In my defence, I can’t bear to! Do your research.)
Now, this is pretty desperate stuff. Rather than recognise the possibility that there are other causes for increase of a variant besides vaccine, it is enough that a vaccine has been used, on however small a number, within a few hundred miles of the epicentre!
Selection requires a differential in output. If one variant produces exactly the same number of secondary cases (on average) than another in the same environment – if they possess the same R value, in epidemiological terms – there is no opportunity for selection. It cannot increase relative to the other (by selection) without a differential it can affect: to get into more bodies it must have the greater R.
The role of vaccine effectiveness
Now, this selective advantage can only happen even in principle if the efficacy of the vaccine against infection (VE(i)) is greater than zero. Efficacy in ideal conditions represents the differential between a vaccinated and an unvaccinated group of the same size and composition, where no-one knows which group they are in. In real world use, the term ‘effectiveness’ is used instead of ‘efficacy’. In the real world, people know if they are vaccinated or not, affecting behaviour, and it also becomes more difficult to equalise groups with respect to other differentials such as age, comorbidity, socioeconomic factors and so on. Because of this – news though this will be to countless amateur internet data analysts – you cannot naively count cases in the two groups, and claim this accurately captures VE.
So, an accurately determined VE(i) gives the percentage differential in case count between treated and untreated groups of equivalent composition. 100% effectiveness means no cases in the vaccinated group, 0% means an identical (or a statistically insignificant differential in) case count. Intermediate values give the percentage reduction – eg 40% VE means 6 cases in the vaccinated for every 10 in unvaccinated: a 40% reduction. From this and the above, then, it is clear that VE 0 cannot generate vaccine escape – there is no possibility of getting into more bodies if the vaccine is completely ineffective; there is no selective pressure if it doesn’t work.
But the relationship is not simply dichotomous. The strength of selection in the vaccinated, minimal when VE is zero and maximal when 100%, must therefore vary continuously between those extremes. The phrase “does not stop you catching it or passing it on”, regurgitated monotonously online and whenever anyone sticks a microphone in front of a sceptic, means only that VE(i) is less than 100% – whereas the intent of most regurgitators is to suggest VE(i) is therefore zero, and there are exactly as many cases in a vaccinated as an unvaccinated group.
It is true that VE(i) is steadily going down, due to waning, antigenic drift and the generalised immune escape of variants. Many even claim (based on shoddy VE-hacking by those amateur analysts referenced above) that VE(i) is negative for omicron.That being so would mean that omicron, at least, is not the variant vanden Bossche is looking for.
For how can it select for immune escape if it confers no immunity?
We can extend this argument backwards. Each variant going forwards has successively diminished VE(i) – and, as the ‘does not stop’-ers continually remind us, immunity wanes anyway. Therefore, Vanden Bosschian Selection must have been getting steadily weaker as a force, if it ever existed. But because Crawford has managed to locate a handful of vaccinees in the vicinity of each step, he gives them the same assumed selective force as ‘wild-type’. I’d bet a pound to a peanut that Crawford and Weinstein have been pushing the implicit-0% “does not stop” narrative throughout 2021 (God forbid anyone should have a reason outside themselves to get jabbed!). And yet, a classic have-cake-eat-cake scenario, they also argue as if selective power were maximal throughout the series. No waning, no antigenic drift.
It is interesting to see how doggedly people have been pursuing the absolutist “does-not-stop” line, and they seem almost relieved that omicron and waning have come along to retrospectively justify the falsehood they have been pushing throughout 2021. “It’s going down” is a tacit admission that it was once up, no? But you’d have struggled to find a sceptic able to concede that in mid 2021. To concede it would kick one of the legs out from under their no-vax-‘cos-I’m-OK stance. Yet the graphs they gleefully point to now show clearly that, when they were vigorously arguing against there being any protective effect whatsoever, there quite clearly was.

Sure it wanes. But you don’t start off waned. Anyone commencing a course now will not have to worry about waning for a good while. Regarding waning as a justification for not getting jabbed is akin to regarding a motor vehicle’s Certificate of Roadworthiness as unnecessary, since it will expire next year. On the other hand, anyone who had the disease in early 2020 may have little protection left; renewal may be appropriate.
The role of frequency
Ignorance of diminishing VE is not even the main thing wrong with Crawford’s analysis. If we assume, for argument’s sake, that a variant can gain a copy specifically by infecting a vaccinated person, and these are rare, how is this supposed to translate into widespread transmission? The individuals in these trials were jabbed then went back to their communities, spread out; little pinpricks in the broader ground of unvaccinated individuals. Our variant gets an extra copy from infecting such a vaccinee, but it may have a long wait to find another. Remember that it only gets an advantage in vaccinees, in this example. The rest of the time, it wanders round the unvaccinated in direct competition for bodies with its ancestor, against whom it has no advantage. So this restrictive scenario isn’t going to work.
OK, you say, let’s give it an advantage in the rest of the population too. Perhaps it can evade innate immunity, or evade the immunity of the previously infected. Indeed it might, and does. But now, we have abandoned vaccination as a unique cause of selective advantage altogether. If we create a selective advantage outside of vaccinees, that could easily be a prime driver itself – especially if there are far more such individuals. It doesn’t speak well of Weinstein’s grasp of evolutionary biology that he failed to notice this effect of the rarity of the advantageous circumstance on the strength of selection.
This is what we see in practice. The variants thrown up so far do not differentially ‘prefer’ vaccinees. They are simply hyper-infectious, and evade innate, infection-acquired and vaccine-induced immunity with not much discrimination. Such discrimination as does exist appears to give greater advantage, if anything, to escape of infection-acquired immunity. This is the opposite of what is needed; people can’t argue that ‘natural immunity generates fewer cases’ at the same time as arguing ‘vaccines select more strongly’.
The role of mutation
Mutations do not necessarily arise where they find their advantage. They are a function of number of replications – the more infections there are, the more opportunity for mutation. Once arisen, mutations are metaphorically chucked against the wall to see if any stick. Outside of hosts that provide an advantage (in terms of additional bodies entered), they can only drift. Once they hit the right kind of host, they get a boost, and if there are a lot of such hosts, they get a lot of such boosts. This can be enough to drive out and replace the ancestral type, where ‘the right kind of host’ is common. But consider: if there were a way of reducing the number of replications, that would reduce the number of mutations. Do we have such a way? Well, yes. Vaccination. Sure it’s not perfect. Sure it wanes. But it will help limit the problem. If people who spent last year arguing against the protective effect had instead embraced it, we might be in a better position now Even 20% effectiveness against infection is protective – 8 cases per 10 unvaccinated, instead of 10. That’s two individuals not passing it on who otherwise would have. And because, unlike additive parameters like hospitalisation and death, the effect compounds, the benefit goes beyond one generation. With an R of 2, after 1 interval we have 16 instead of 20. After 2 we have 32 vs 40. After 3, 64 vs 80, and so on. And of course, the presence of other vaccinees in the population reduces that R anyway. Every little helps.
There’s another possibility, and that is someone involved in collecting bats got infected and brought the virus back without bringing back the source bat.
The point that no one has undermined is that bats were not on the menu and not for sale in Wuhan wet markets.
But, the discredited scenario continues to dominate popular discussion, and few peer reviewed papers mention the difficulties.
“ Live-animal markets promote inter-species contact among wild species, domestic animals and humans. In fact, the epidemiological evidence indicates that the spillover of SARS-CoV-2 to humans was associated with close contact between humans and exotic animals, most likely in Chinese wet markets. ”
https://link.springer.com/article/10.1007/s11259-021-09787-2
But there are some:
“ Not surprisingly then, the finger of blame has been pointed at wildlife trade in the wet markets of Wuhan, Hubei, China, where this Covid-19 outbreak seems to have originated.
…
With these huge concentrations of diverse species under one roof, while we discovered no evidence supporting original spill-over from candidate bats or pangolins in Wuhan, it would seem but a matter of time before some other unwelcome disease might skip into the human population. ”
https://www.ox.ac.uk/news/science-blog/wet-market-sources-covid-19-bats-and-pangolins-have-alibi
Just a modest request. Could we have a discussion of the possibilities, without name-calling?
?que. la cabeza funciona finalmente?
Good for you dazz!.. you are coming to your senses.. though gradually
What made you think I care?
BTW: I’ve move on. ID is not my primary focus anymore. I may do a piece on what I have been doing for the last 20+ years but I don’t really care anymore..
I’ve been in touch with some of the top ID guys and they have not new ideas, I’m afraid..
How did the furin cleavage site get inserted via well known evolutionary mechanisms?
You are not a religious man, right?
That’s not the problem.
Splendid risk assessment by Canadian anti-vaxers:
Michelle Goldberg, “The Giddy, Terrifying Siege of Ottawa,” The New York Times
Free access (limited time), Ordinary link
I think we can say that public health measures can cause harm, and at the same time be justified. But people may differ in their weighing of benefits.
CDC has just adjusted the milestones for language development by six months. I’ve seen an example of language delay in my relatives. A grandson and grand nephew who didn’t start talking until recently, when they started day care. They have spent most of their first two years without age mates.
This makes me think about a language development discussion on another forum. Some kids seem unwilling to engage in baby talk, and don’t start talking until they can master sentences.
I’m now curious whether this has anything to do with being around adults rather than other kids.
We’ve just done a forced experiment in child rearing. Without the pandemic, depriving toddlers of socializing opportunities would have been called abuse.
petrushka,
Social distancing has changed how folks greet each other here. Prior to Covid, a handshake was obligatory on all meetings and friends and relatives got a kiss on both cheeks, no matter if man/woman, man/man or woman/woman. Just a knuckle tap now.
But I’m an optimist. Looking at the falling infection rates, I think we might be turning a corner at last, no small thanks to the vaccines.
Really? You think every child over the past 10,000 years that was was raised in a rural environment with few neighbors nearby is an abused child? They are all deranged?
Its a pretty long experiment which would suggest otherwise.
Wyoming, how could you?
Deliberately depriving a child of playmates unnecessarily sounds borderline. I grew up in the kind of rural environment you describe. I can’t say I’m ruined, but I’m pretty introverted.
I’m also optimistic, but I think the future belongs to antivirals. Eighty million Americans have tested positive, officially. Unofficial CDC estimates would put the actual count at three times that. Add in vaccinations, and just about everyone has been “trained”, exposed or infected. “Healthy” people are not at high risk of dying.
I think just about everyone in the world will eventually be infected. Probably more than once. I hope antivirals will bridge the gap for people with weak immune systems. The price will come down. They will be used to prevent infection and block transmission.
Oh the horror.
23 of the Most Amazingly Successful Introverts in History
This generation may be doomed. Think of all the frats parties that might never be.
I grew up in a well populated neighborbood. Nevertheless, I am an introvert.
Hmm. Binarism again. I don’t believe it is possible to categorize people as either introverts or extroverts.
There are 10 kinds of people.
Alan Fox,
There are people who think life is binary and people who don’t.
Oh, you are one of those.
Dr. Vincent Racaniello on antivirals:
That’s just silly. If you are a high risk person — particularly a person in long term care, you get tested at first symptoms, and start the antivirals immediately.
One of the features of omicron is the first symptoms appear before lung involvement. I believe you have several days to start treatment.
Of course, availability is severely limited, but that will change. My wife waited two months for the vaccine, but now you can almost walk in.
In the long term the price will go down, and there will be competition.
If they block transmission, they will be taken as a preventive by people exposed. Perhaps the full course isn’t necessary as a preventive. Covid will be around a long time. We will learn.
I don’t know if this is legal, but I know from direct observation, that doctors will prescribe some medicines that you can keep on hand, just in case.
The treatment for Lyme disease is two or three weeks of antibiotics. But a single dose will prevent infection if taken within 48 hours of a tick bite. I have a supply of those single dose preventives.
With so many asymptomatic cases, I’m guessing antivirals wouldn’t be very effective at slowing down transmission, unless they’re used preemptively. Racaniello also said that in that scenario, we would need at least two or three different antivirals to avoid having the virus develop resistance to it.
Right now there doesn’t seem to be a single one of them tested for efficacy nor safety. So, will it be really cheaper than vaccines to develop, test and produce several antivirals that have to be administered periodically, or should we focus on developìng a vaccine that protects long term and works for all variants? Racaniello thinks it should be possible to do the latter, with a vaccine that produces antibodies for the stem of the spike instead of the tip.
Racaniello also mentions that: he says even though these antivirals are untested, they’re FDA approved and doctors can prescribe them off-label.
If anti-vaxxers want to be the guinea pigs who test these drugs for us all, it’s up to them. Would be kind of ironic, considering their “vaccines are experimental” narrative, but hey, it’s a free world, right?
No, not silly, merely out of date: that video dates back to September.
The first anti-viral approvals were restricted to hospitalized patients — e.g. Veklury (remdesivir) was originally (10/22/20) restricted to hospitalized patients.
Only more recently have anti-virals been approved for mild-to-moderate patients at high risk: remdesivir on 1/21/22, and EUAs for molnupiravir [which is highly effective] and Paxlovid (nirmatrelvir+ritonavir) [not so effective] in December 2021.
The “fill the prescription now, in preparation for getting ill” approach has been in use for decades, in particular with Tamiflu, where early intervention is key.
ETA: Aaargh! I got the efficacies backwards: it’s the protease inhibitor (Paxlovid) that appears to work better…they are all powerful drugs with potential side effects.
It turns out, people are morons. Lots of people won’t get vaccinated, and would rather wait to get infected and then take the [more dangerous] anti-viral.
From a public health standpoint, it’s a disaster.
For Merck and Pfizer, it’s a windfall. (And yes, they’ve done the market research…)
Oh, so I was wrong on that. Good to know, thanks!
My understanding Is wit omicron 2, just being in the same room with a infected person is sufficient. Hong Kong lasted two years, but has succumbed to one or the other omicrons.
Everybody will get it. Most anti-vax ears are young, and 99 percent will survive.
The place where antivirals are needed as soon as available are in nursing homes and for immunocompromised people. If covid mutates in such people, antivirals might reduce the number of variants.
We are approaching a phase where the virus will be in continuous circulation somewhere in the world, and people will stop thinking of it as life threatening. Since vaccines are not stopping the spread, antivirals might slow it.
There’s lots of confusion about how likely it is for asymptomatic people to spread the virus. There’s evidence that the answer is lots less likely.
Wholly caw. I need to pay attention to autocomplete.
Don’t forget long COVID either. Many are still dealing with ongoing debilitating symptoms.
On the extrovert/introvert thing, my serious point is there is both a spectrum and where you are on the spectrum can change, in my case sometimes within seconds.
I can interact with a few people at a time, but at a party, or a large group, or an audience, there’s no hope.
Lots of common products, including Tylenol, or peanuts, can kill you.
I would guess within a year, we will know how safe paxlovid Is, and under what conditions. I’m going to guess that for high risk people, it is safe enough, and we will learn about drug interactions pretty quickly.
https://www.biorxiv.org/content/10.1101/2022.02.14.480394v1
The fact that the CDC felt the need to change the definition of a vaccine tells you all you need to know about the efficacy of the co\/id shot. It was never a vaccine to begin with. No flu shot has ever risen to the high bar of vaccine status. The co\/id shot is no different. Changing the definition did diddly squat to change that fact.
Oh, but it reduces the symptoms I hear you all saying? Well, eating right like eating lots of greens and fruits does the same. It always has against the flu. Nothing different with co\/id.
So what’s all the hysteria about? Im unvaccinated and I prolly got co\/id some time or another but have no way to know. I mean ive gotten slight sniffles in the past couple of months. But there was this strange incidence though.
I and my wife were around fully vaccinated extended family at a holiday get-together (5 days total) and we both got swollen feet (she is also unvaccinated-not because she doesn’t think its a good idea but just because she hates needles and doctors as a general rule-thank god for that). The weirdest thing. It lasted about a 1/2 day. The swelling went down the next morning. Then it happened again after another day and again went down quickly. I suspect it was the shedding from the vaccinated but no way to know for sure.
Im 58 and in a supposedly higher risk group. But I have been giving myself and my wife a dark green juice blend (spinach, green pepper, celery, wheatgrass powder) with added D3, zinc, iodine, and C for several weeks. So got everything including K from the wheatgrass.
Aaaaahhhh… could that be the reason our feet recovered from the swelling so fast? Seems our bodies took care of the shedded spike proteins in the same way Trudeaus goons took care of Canadian truckers and bystanders.
Whatever the case may be, seems the co\/id shot has always been an unnecessary distraction. A risky one at that!
Actually, there’s an easy way to be pretty certain: if your symptoms were caused by spike shedding, you should be seropositive for anti-spike, but seronegative for anti-nucleocapsid. You can confrim your suspicions with a pair of simple antibody tests.
My money’s on the salty snacks, though.
This is what comes of cherry-picking convenient anecdotes, while VERY carefully avoiding the widely published statistics. And it remains the case that those who have had the sense to get vaccinated are OVERWHELMINGLY outnumbered by the unvaccinated when it comes to confirmed cases, hospitalizations, and deaths.
As far as I’ve been able to tell, the jury is still out on what causes some (perhaps a minority) of infected people to become very sick, or die, or suffer “long covid” from internal damage the virus caused that cannot be corrected — while others, as Steve says, would never know they had any infection if they were not tested. Some epidemiologists are now saying that the recent drastic decline in cases could be a matter of actual herd immunity – the virus has already infected enough people that it’s running out of the sort of victims whose systems could cause them to become statistics. But meanwhile, confirmed cases are still increasing in some places. Today I read that was true in Connecticut, Pennsylvania and North Dakota. Notably, these increases are with few exceptions among the unvaccinated.
As for the vaccination itself being risky, this is simply flat false. Yes, there are some people who react badly to it – perhaps one or two per million people. Which is no worse than inoculations for the flu, or smallpox, or MMR. Compare with the roughly one in four (that is, 250,000 per million) unvaccinated who get covid. A healthy diet probably makes for a more robust immune system, but it is NOT a cure for covid or any other virus.
The facts haven’t changed — anyone’s best chances come from getting the vaccination and booster, wearing masks, avoiding indoor crowds, and washing hands. Oh, and from NOT becoming an anti-vax podcaster or radio host.
LOL, I was also immediately thinking of pets or other sources of an allergic reaction.
Flint,
You misunderstand. There is NO cure for co\/id like there is no cure for the flu.
By the way, they are the same thing. Isnt it remarkable that in 2019-20 there was what, some odd 30M+ cases of the flu and all of a sudden in 2020-21 there are what, 1800+ cases? So the flu magically fell of the face of the earth? puleez!
Oh and your omitting to tackle the question of the shots being a vaccine or not did not go unnoticed. Would you like to tell us just how these shots are considered a vaccine using the original definition that has been used for what 80 years now? why the sudden desire to modify the definition of what a vaccine is?
You (pl) take people for fools. its laughable.
Oh, and masking kids that have the most robust immune systems and easily handle co\/id. what kind of fuckery is this?
Well no need to fork out any bucks to confirm suspicions. We are healthy, unvaxxed, and going strong. No irrational fear of a scary sounding version of the seasonal flu.
But we do thank Gates for the heads up that another pandemic is on the horizon. We will surely need a running start for that one.
Being an anti-vaxxer in a high risk group, I don’t think you need anybody else to make you look foolish.
It appears ignorance about modern diagnostics has taken on epidemic proportions. I have analysed hundreds of SARS-CoV-2 sequences by now and they do not resemble influenza at all. You are talking nonsense.
Only when they act like fools. I will be thinking of you and your spinach drink when I am enjoying my beer this weekend.
Steve seems strangely incurious. I am certain that he could raise the funds a thousand times over with a GoFundMe campaign: two antibody titres and he will have demonstrated that Covid vaccine shedding is real! He’d be the hero of the GOP! The darling of Fox News!
But at least he is not succumbing to “irrational fear”.
LOL
https://www.sciencedirect.com/science/article/pii/S193131282200049X?via%3Dihub
On the subject of neutral or helpful viruses.
Where did you get the idea that I was anti-vaxx? the co\/id shot is not a vaccine. does it prevent the flu. No. ’nuff said.
Tweaking a word’s definition to allow co\/id in the vaxx club is pretty lame.
And here I thought I was dealing with rational people on TSZ.
Why would anyone want to fork out money to confirm if it was indeed sheddding or not. My swollen feet healed in 24 hours. As did my wife’s. I certainly didnt claim that indeed it was the result of shedding.
However, the coincidence of two un(faux)vaxxed people in a room full of (faux)vaxxed people for 5 days straight and the two (faux)vaxxed people getting thrombosis would tend to lead to an educated guess that shedding was indeed a possibility.
For the record, my wife didn’t believe it. She thought the thrombosis was caused by the homemade pork sausage that her sister made. Besides my speculation that it was the shedding, homemade pork saugages were the only other possibility.
So if my wife is right, then I guess there is something to be said about getting a co\/id shot. You don’t have worry about getting sick from homemade pork saugages lol.
Congrats to you Corneel on your hard work analyzing sequences. For the record I have surely not tried to diagnose anything. It was simply an straight forward observation people have made. You have to admit that it is quite curious influenza seems to have been ‘cured’ and replaced by SARS-CoV-2 .
How does that happen? Our masks and social distancing and lockdowns stops influenza in its tracks but SARS-CoV-2 just ran roughshod over our elaborate precautions???
Im glad you will be thinking about how I allow natural substances to course through my veins quickly healing thrombosis, preventing co\/id and influenza at the same time. All on the cheap to boot. lol its gonna be another great day.
Oh, and to put some more salt in that beer you will be having…..ive cooked up some homemade Kombucha. grapefruit, lemons, korean pears, star-anise, and pro-biotics. The pro-biotics when you let the mix sit for a weak creates natural carbonization. and we leave half the fiber in the mix to scrub the intestines for natural cleansing.
co\/id, eat your heart out!
Quite: you claimed that there was no way to know for sure. That was wrong. You must realize that you represent a golden opportunity to advance medical science by demonstrating that covid vaccine shedding is a real thing, yet you seem rather unwilling to put your convictions to the test. Selfish, some might say.
“Thrombosis”? Based on what? You described peripheral edema, not thrombosis. I cannot see how it is an “educated guess” that shedding was a possibility, given that shedding is only an issue for live attenuated viruses.
Really? The only other possibility? In addition to the salt content of those sausages, there’s the “spending way too much time standing and sitting”, which will cause noticeable edema in most people over 55. Such edema is generally gone in the morning…
Better yet, these people don’t believe PCR is a valid means to determine whether you need the antiviral, nor whether or not the antiviral in question has the efficacy they are convinced it has. All based on a 10 second mumble by Mullis. Dickheads.
petrushka,
I never understand why people think 1 in 100 dying is OK.